The most recent installment in my monthly series, published on the 22nd of each month. For prior posts go here.
The situation in the U.S. continues to be bad, though it may be peaking or slightly past peaking in some states.
Europe continues to be hit very hard. Germany, which came through the April/May wave pretty well is currently having the equivalent of 3,000-4,000 deaths a day (based on U.S. population). The next large country which may experience an upsurge in deaths is Turkey which is currently seeing 200-250 daily. Over the past month that country has seen a tremendous upsurge in cases not yet reflected in deaths.
In Asia, South Korea and Japan continue to have very low death rates but during the past 2-3 weeks both countries have seen their highest daily death tolls since the start of the pandemic, though in absolute terms much lower than that in Europe and the Americas.
------------------------------------------------
Now that vaccines are available we can look forward to covid being brought under control over the next 3-5 months (our ER doc daughter was vaccinated yesterday). There has been a lot of discussion about priority setting for who gets vaccinated and when.
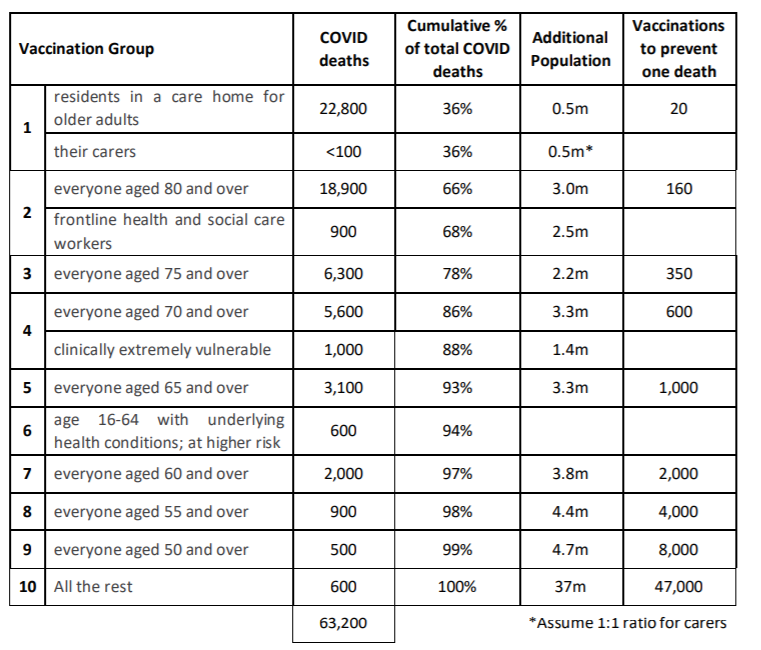
Here's a very sensible one scheme from the U.K. which it describes as representing "around 99% of preventable mortality from COVID-19".
1. residents in a care home for older adults and their carers
2. all those 80 years of age and older and frontline health and social care workers
3. all those 75 years of age and older
4. all those 70 years of age and older and clinically extremely vulnerable individuals
5. all those 65 years and older
6. all individuals aged 16 to 64 years with underlying health conditions which put them at serious risk of disease and higher mortality
7. all those 60 years of age and older
8. all those 55 years of age and older
9. all those 50 years of age and older
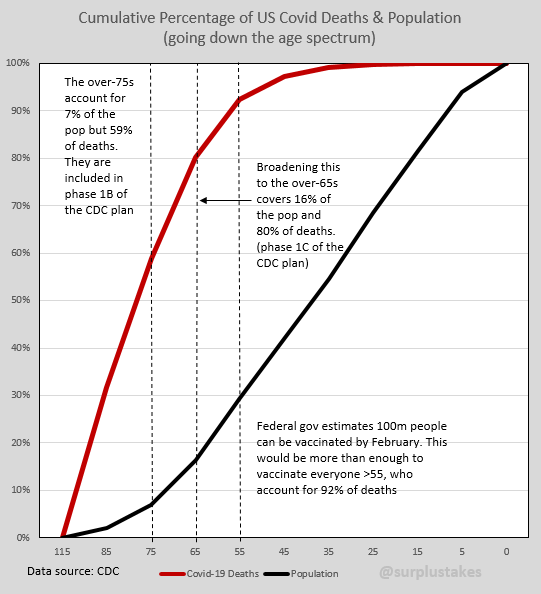
Here's an analysis explaining the UK approach:
The
U.K. plan makes sense if your priority is saving lives. Fatality rates
skew very much towards the elderly with covid. Here's the current U.S.
data showing each age group as a % of overall covid deaths:
85+ : 31%
75-84: 27%
65-74: 22%
55-64: 12%
45-54: 5%
35-44: 2%
25-34: 0.7%
15-24: 0.2%
Along the same lines this is the Arizona mortality rate per covid case by age:
65+: 10.3%
55-64: 2.3%
45-54: 0.8%
20-44: 0.2%
< 20: 0.02%
What this means is if you get covid and are 65 or older your chance of dying is 51 times that of someone between 20 and 44 who has covid. NOTE: If Arizona broke its 65+ data down in more detail you would probably see something more like a 5% rate for those 65-74, 10% for 75-84 and 20% for those 85+.
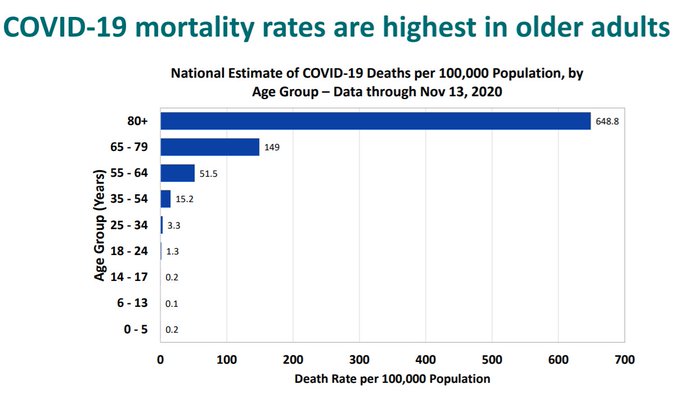
A way to visualize the differential risk by age:
Another example of age and health differentials can be seen by comparing mortality data for U.S. military personnel with that of Veteran's Admininstration patients. The fatality rate per confirmed covid case for the younger and healthier military personnel is 0.11%, while for the older and health impaired VA patients it is 4.33% or nearly 40X greater.
There is an alternative methodology to that selected by the U.K. which would focus on years of life saved. For instance an 85 year old may have an additional life expectancy 4 years, versus an 40 year old with 40 years of life expectancy. Who should get priority for the vaccine? I don't think the arguments are as strong as that in an age-based scheme because the death rates skew so dramatically with covid, but it is an argument at least worth thinking about.
Unfortunately the United States seems focused on other factors, at least in part, which led to the flawed recommendations made on Sunday by the CDC Advisory Committee on Immunization Practices (it now goes to CDC Director Redfield for a final decision). According to Stat News, the panel recommended the highest priority for those in long term care and health care workers which makes sense, with the second priority to those 75 and older and frontline essential workers, which makes less sense, and the third priority to those 65 and older, people 16 to 64 years old with high-risk medical conditions, and essential workers not included in the second phase of vaccination, which makes even less sense, if the priority is saving the maximum amount of lives. It turns out that was not the Committee's highest priority.
Here's an alternative approach, rejected by the "experts".
The first problem is the size of categories the CDC and Committee is using which is going to lead to a lot of confusion and infighting, particularly because they contain 202 million people (60% of U.S. population) and there will only be about 100 million vaccine doses available before March (24 million in Phase 1a, 49 million in Phase 1b, and 129 million in Phase 1c). This is how academics decide things, not people with practical experience on implementation. The U.K. approach takes much smaller slices of population in a clearly understandable sequence, and should be much more manageable.
But the real problem is when you try to answer the question - why would the CDC committee recommend a priority list that would result in more deaths? The answer is the injection of Critical Race and Social Justice Theory and into public health decisions.
Frontline essential workers are defined as:
"first responders, teachers and other education workers including day care workers, food and agriculture workers, correctional facility staff, postal workers, public transit workers, and people who work in manufacturing and in grocery stores"
And Stat News quotes Peter Szilagyi, a committee member and pediatrician at UCLA;
“I voted for this recommendation because in my opinion, it follows the evidence about the risk from coronavirus and the ethical principles that we have developed on ACIP to maximize the benefits and minimize harms, promote justice, and to minimize health inequities. We are trying to thread the needle here.”
Stat News goes on to mention the lone dissenter to the committee recommendation:
Henry Bernstein, a pediatrician and professor at the Zucker School of Medicine at Hofstra/Northwell, said he felt that adults aged 65 and older should have been in Phase 1b. The toll the virus takes on people 65 to 74 is not substantially different from its impact on people 75 and older, he argued.
So, what's going on here? Bernstein's position is very clear. If you look at risk and lives you save many more lives by including 65-74 year olds in Phase 1b.
But what, precisely, is Dr Szilagyi saying? He's rambling about "ethical principles", "justice" and "health inequities". That's just jargon. What does it mean in practice? Why can't he say what he means as clearly as Dr Bernstein? It's because he trying to obscure what he means.
Let me translate. What Dr Szilagyi is saying is, "because blacks are a disproportionate amount of essential workers, and are at disproportionate risk, it is inequitable to give them lower priority on the vaccine, so older people must be lower priority and more of them die, including those at most risk, black seniors, in order to be equitable." Please don't mistake talk of "equity" for that of "equality". Equality is treating people equally, though the may eventually have different outcomes in life. Equity means that any difference in outcome for a minority is attributable to white supremacy, is therefore racist, and society must be adjusted to correct that outcome.
Yes, I know it doesn't make sense but that's the way these social justice people think, and now you know why he won't say it clearly. When Dr Szilagyi says, "We are trying to thread the needle", he is referring to designing a system in which more people die than necessary but which, in his calculation, is fairer racially and, at the same time, obscuring what they are doing.
To understand how the committee came out here, it is important to note that the CDC "experts" originally were going adopt an even worse alternative. This was their original draft analysis. First they looked at science and implementation and the 65+ category came out ahead:
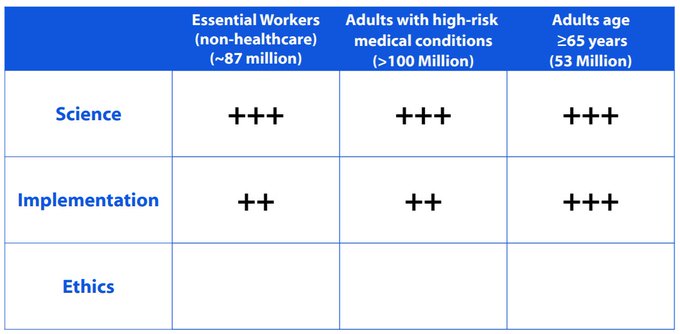
Ah, but then come Ethics!
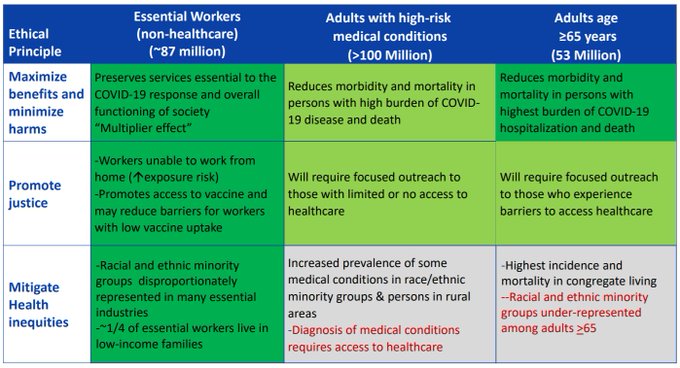
And suddenly, non-healthcare essential workers are ahead!
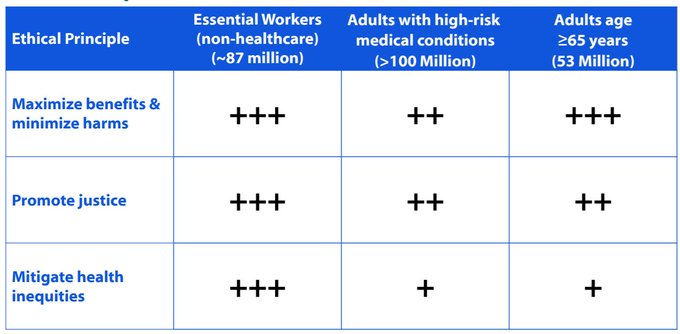
So, the original recommendation was that essential non-healthcare workers get priority over anyone who was over 65 and not in long-term care. And, as one commentator noted:
"Incidentally, this report has many classic bureaucratic hallmarks: - the spurious symmetry of three equally weighted categories, each with sub-categories - the erratic marking thereof - the artificial separation of "Ethics" and "Science" - the opaque and questionable modelling"
This leaked and the blowback was so severe the committee agreed to extend priority to the over 75 crowd, even though substantial lives could be saved by lowering the age to 65. No surprise, the New York Times found a bioethics "expert" (bioethics, by the way, is an immoral academic field) to opine that more elderly white people needed to die in order to provide equity.
Not to be outdone, Marcella Nunez Smith of Yale's School of Public Health, and co-chair of Joe Biden's newly announced COVID-19 Advisory Board, complimented the CDC experts for "taking political interference out of the process" and for their "grounding in inequity". Huh? They took science out of the process and injected ideology. These people are dangerous. Americans will die because of them.
[IMPORTANT ADD: Just after publishing this post I came across an article by Aaron Sibarium at the Washington Free Beacon, "How the Centers for Disease Control went Woke", which is worth reading in its entirety. It provides additional background on the vaccination priority process and how Critical Race Theory informed it. A couple of excerpts describing how Wokeness distorted the process:
The result was a kind of moral double counting, in which closing disparities promoted two separate values, whereas saving lives promoted just one. As phrased, equity and fairness sound like they are at odds with harm reduction: If vaccinating by age minimized deaths across all racial groups, but widened the gap between racial death rates, the principles seem to rule out that strategy, since it would increase racial disparities overall.
The CDC also expressed concern that vaccinating by age would amount to immoral—and potentially illegal—discrimination. The evidence its experts cited, however, arguably favored doing just that.
One graphic from Oliver's presentation, used to illustrate the trade-offs of prioritizing the elderly, cites a statement from the American Geriatric Society that "age should never be used to exclude someone from a standard of care, nor should age ‘cut-offs' be used" to allocate scarce supplies.
The CDC committee thus took two statements that championed the interests of the elderly and used them to justify a plan that would disproportionately kill senior citizens —implying that age-conscious alternatives were discriminatory, even as the race-conscious plan passed with unanimous support at a subsequent meeting.
All of this—the exclusions, the contradictions, the moral redundancies—helped disguise the agenda that it justified, giving unscientific value judgments an air of scientific assuredness.]
FURTHER ADD: I came across this piece by stalwart liberal Yascha Mounk describing the moral depravity involved:
". . . there are also some bedrock principles on which virtually all moral philosophers have long agreed.
The first is that we should avoid “leveling down” everyone’s quality of life for the purpose of achieving equality. It is unjust when some people have plenty of food while others are starving. But alleviating that inequality by making sure that an even greater number of people starve is clearly wrong. The second is that we should not use ascriptive characteristics like race or ethnicity to allocate medical resources. To save one patient rather than another based on the color of their skin rightly strikes most philosophers—and most Americans—as barbaric. The Centers for Disease Control have just thrown both of these principles overboard in the name of social justice.
In one of the most shocking moral misjudgments by a public body I have ever seen, the CDC invoked considerations of “social justice” to recommend providing vaccinations to essential workers before older Americans even though this would, according to its own models, lead to a much greater death toll. After a massive public outcry, the agency has adopted revised recommendations. But though these are a clear improvement, they still violate the two bedrock principles of allocative justice—and are likely to cause unnecessary suffering on a significant scale.
Since states will now have to decide whether to follow the CDC’s recommendations, the fight for a just distribution of the vaccine is not yet over. At the same time, the past days have already taught us two lessons that sum up some of the most worrying developments of the past years: The attack on philosophically liberal principles has by now migrated from leafy college campuses to the most important and powerful organizations in the country. And, in part as a result, it is getting harder and harder to trust institutions from the CDC to the New York Times."
Everyday I am more convinced that getting rid of the poison the Woke are injecting into American society must be the #1 priority for decent Americans.
Now let's look more closely at the definition of the frontline workers to be included in Phase 1b. First responders mean police and firefighters, not EMTs. My comment two paragraphs below covers them.
But why teachers? We've known since summer that schools are low risk for covid, both for students and teachers. And unlike the others in this category who've been working since the start of the pandemic, most teachers have not been working in person and their unions have been insistent on keeping schools closed despite the science.
The other categories also contain significantly lower mortality risks. In some instances, for instance meat packing plants, we've seen major case outbreaks but with very low mortality rates. Moreover, we have now gone for nine months with covid, with essential workers not having access to vaccines, and our supply chains have not been disrupted (to my surprise but it is true).
If the mortality demographics of covid were different there might be a case for prioritizing groups with lower mortality but who can transmit to more those more vulnerable on the theory that transmission chains can be broken. But the covid mortality rates above 65 are so much higher than for those younger that strategy would take much longer than direct vaccination of the vulnerable.
A UK strategy, stratified for age in smaller groups, would also capture those essential workers below 65 who have dangerous conditions which may cause issues if they get covid.
The good news is that the CDC just make recommendations and each state can set its own priorities. Texas has just announced its priority approach which is closer to that of the UK than of the CDC committee. Other states are taking the social justice mantra even further - Massachusetts is prioritizing prisoners over elderly not in long-term care and those of any age with two or more comorbidities.
ADDED: One final note. There is a glaring inequity that is being studiously avoided in the discussion of covid impacts.
Of those older than 85, about 60% of deaths are of women. This is not unexpected as the average lifespan for women is five years longer than for men (81 years v 76 years), the first inequity we encounter.
But, according to the most recent CDC data, of those who have died from Covid and are less than 85, 60% are men, a figure far outside the normal range, indicating that the coronavirus is hitting men much harder, the second inequity.
-------------------------------------------------
Seven of the eight countries I predicted last month would pass 400 deaths per one million population have done so (Poland, Portugal, Austria, Hungary, Croatia, Georgia, Costa Rica). The exception is Tunisia (357) where the current wave has slowed down. Of the four countries predicted as possibly passing 400, only one (South Africa) had done so, though Ukraine will surpass 400 in 3-4 days and Canada in about 10 days.
Two other countries joined the 400 club - Greece (417) and Lithuania (404).
Eight more countries will surpass 400 in the next month - Costa Rica (398), Ukraine (387), Albania (386), Canada (381), Russia (356), Germany (337), Serbia (319), Slovakia (296), and Latvia (245). Paraguay (296), Tunisia (357), Jordan (354) and Azerbajian (225) may also join the list. By next month the only European countries not to be over 400 will be Finland, Norway, Denmark, Estonia, and Belarus (I don't place much credibility in data from that last one).
And, on any given day, about three dozen countries are exceeding 1,000 deaths if scaled up to U.S. population levels.
NOTES:
1. I originally picked 400 as a marker when the U.S. rate was lower (688) and because of the wide variability in how each country determines covid deaths. It is misleading to do direct comparisons and we really have no idea if one country with a reported rate of 700 is different from a country reporting 800. For consistency's sake I will stick with 400 as the benchmark, but if you are looking for comparisons to the U.S. I would look at 600 and up.
2. This list only includes countries with populations in excess of one million.
3. In predicting which countries will pass 400 I'm not doing modeling or statistical analysis. It is based on my gut feeling having watched daily data for several months.
4. A per capita rate of 400 means 0.04% of the population has died from covid; a rate of 1000 translates into 0.1% of the population.
5. The countries are shown below by continent, listed from highest per capita mortality rate to lowest. In parens are indicated the rates for the past 3 months (Oct/Nov/Dec). A - is used to denote a month where the rate was below 400. Countries new to the list are shown in Boldface.
Europe
Belgium (908, 1337, 1610), Slovenia (-, 506, 1163), Bosnia & Herzogovina (-, 695, 1159), Italy (612, 825, 1156), North Macedonia (420, 714, 1123), Spain (738, 911, 1059), UK (652, 809, 1004), Bulgaria (-, 416, 994), Czech Republic (-, 668, 985), France (524, 746, 944)), Hungary (-, -, 877), Croatia (-, -, 813), Sweden (586, 633, 806), Switzerland (-, 467, 797), Romania (-, 524, 763), Moldova (407, 533, 696), Netherlands (404, 518, 620), Poland (-, -, 614), Austria (-, -, 613), Ireland (-, 408, 437), Greece (-, -, 417), Lithuania (-, -, 404)
North America
USA (688, 792, 999), Mexico (676, 783, 915), Panama (599, 681, 836), Costa Rica (-, -, 401)
South America
Peru
(1026, 1074, 1121), Argentina (607, 816, 931), Brazil (732, 794, 883), Chile (720,
786, 845), Colombia (581, 691, 800), Bolivia (730, 759, 785), Ecuador (705, 744, 785)
Africa
South Africa (-, -, 423)
Asia
Armenia (-, 658, 901), Iran (-, 531, 639), Georgia (-, -, 547)
NOTES: India, with covid per capita mortality rate of 106, has 146,000 covid fatalities or 8.5% of global deaths.
India and China, with 36% of the world's population, have 9% of covid deaths, meaning 91% of deaths are distributed among the other 64%.
No comments:
Post a Comment